You want to be a Royal Marine Commando?
Introduction
The thirty-two week Royal Marines (RM) training course is recognised as one of the most arduous military training programs in the world (1). The course is both mentally and physically challenging, with approximately 16% of recruits sustain an injury (2), and only 54% of candidates actually completing the course (3).
Other international military personal can attend the All Arms Commando Course (AACC). This is a 13 week course at Commando Training Centre Royal Marine (CTCRM), with the aim of preparing Navy, Army or Air Force personnel for service with 3 Cdo Bde RM by developing the temperament, mental resolve, physical robustness and core military skills necessary in the demanding environment of expeditionary and littoral operations.
The accepted definition of RM fitness is “...an individual with excellent aerobic endurance combined with good upper body strength” (4). The closest correlation in athletics would be a decathlete (5). The closest correlation in athletics would be a decathlete (5). In context this is an athletic event taking place over two days, in which each competitor takes part in the same prescribed ten events (100 metres sprint, long jump, shot-put, high jump, 400 metres, 110 metres hurdles, discus, pole vault, javelin, and 1,500 metres). Throughout RM training, there is greater improvements in strength compared to endurance, therefore it was recommended in an Institute of Naval Medicine (INM) report that greater emphasis (during selection), should be placed on having adequate VO2 max to complete high aerobic capacity tasks (6). Basically you need a set of lunge before you start!
Needs analysis: How Fit do you need to be?
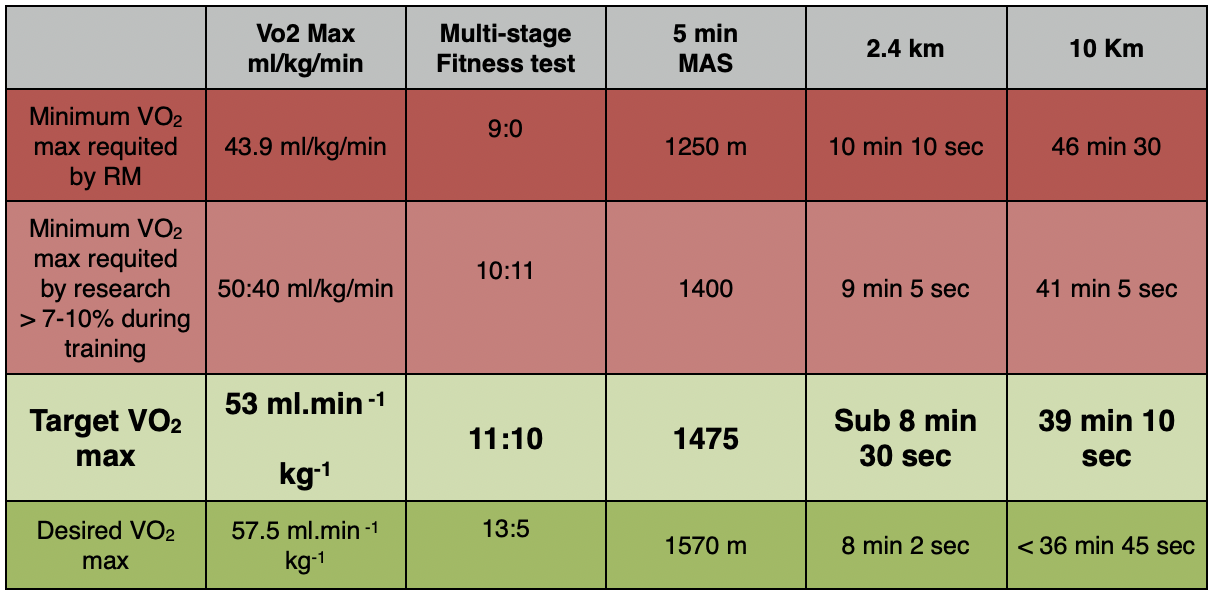
One of the criteria tests of RM training is a 9-mile speed march carrying 15 kg in 90 minutes (The 9-miler). The predicted metabolic oxygen demands for a male to of carrying 15 kg and running 9.7kph (10 min mile) is 40 ml.min -1 kg-1 (7). To complete the 9-miler maintaining an intensity of 75% of VO2 max for the duration of 90 minutes, the candidate would require a VO2 max of approximately 53 mL.Kg-1.min (8). In a stimulation of the 9-miler conducted at INM, the average VO2 was 40 ml.min -1 kg-1, with a VO2 max of 57.5 ml.min -1 kg-1 (9). This supports the earlier VO2 max prediction for the 9-miler. (10)
NATO countries report a predicted increase in VO2 max during basic military training of between 7-10% (11). A minimum aerobic capacity to start RM training would be approximately 50.40 ml.min -1 kg-1 (9). You need to be able to run 1.5 miles (2.4km) in under 10 minutes. This would give you a VO2 of 51 ml.min -1 kg-1 . By the time you are ready for the Commando tests your VO2 should be over 57 and your 1.5 mile time under 9 minute. The higher the VO2 max at the start of the AACC, the likelihood of sustaining an injury is greatly diminished (2). The fitter you are the less likely you are to be injured!!! Low levels of physical activity preceding RM training, combined with low VO2 max and cigarette smoking increase the chance of injury (12). DON’T SMOKE!
During the initial physical assessment of RM training, body weight strength-endurance exercises are evaluation. This is conducted either on the Bottom field and is known as the Battle Physical Training (BPT) (8) involve 16 kg of equipment or load carries with 31.2 kg plus weapon (5.5 kg) . Small and lighter recruits are at a disadvantage as they undergo significant decreases in neuromuscular function and have greater cardiovascular strain (1). UK DEF STAN 00-25 (Part 3)/2, recommends a maximum load carriage of not more than one-third lean body weight (13), for a RM to carry 31.2 kg it equates to a lean body mass of 93.6 kg.
Injury Rates
With such a high injury rate (12), it is prudent to increase the structural integrity of the body to deal with the demands of the training. Stress fractures are one of the most common and potentially serious overuse injuries during RM training and AACC, (14) occurring with greater frequency compared to most athletic training programs, the exception being distance running (15). Approximately 5% of all recruits develop a stress fracture injuries (16), with the third metatarsal being the most common site for stress fracture (17).
Stress fracture pathology is believed to be related to exposure to a level of physical stress that includes high intensity, high-volume activity with repetitive loading of the bone without a progressive build up period. Consequently the athlete is unable to adapted to the increase stress (18). Load carrying alter the vertical and horizontal position of the bodies centre of mass, combined with carrying a weapon that inhibits natural arm swing, significantly increase the impact peak and mediolateral impulse of ground reaction forces and have been positively linked to overuse injuries (19).
Specific Statement of Need: Aerobic Capacity
Specific Needs
Increase aerobic capacity (VO2 max) to minimum of 53 mL.Kg-1.min.
Criteria Tests for Entry:
Multi-Stage Fitness Test - 11:10 (53 mL.Kg-1.min)
Pull-ups - 12+
Press-ups - 60,
Sit-ups 85 - (2 mins)
Increase strength to reduce neurological and cardiovascular strain.
Pre-habilitation (non-quantifiable)
Increase bone density,
Increase Bicep strength to reduce risk of bicep tendinosis in early phase of AACC training.
If it was easy everyone would be Royal Marine Commandos! It’s supposed to be challenging but not impossible.
References
1. Fallowfield JL, Blacker SD, Willems ME, Davey T, Layden J. Neuromuscular and cardiovascular responses of Royal Marine recruits to load carriage in the field. Applied ergonomics. 2012 Nov;43(6):1131-7. PubMed PMID: 22575491.
2. Wood AM, Keenan AC, Arthur C, Wood IM. Common training injuries concerning potential Royal Marine applicants. Journal of the Royal Naval Medical Service. 2011;97(3):106-9. PubMed PMID: 22372015.
3. Pullinger N, Pethybridge R, Allsopp A. Identifying, at selection, the physical and mental characteristics associated with successful completion of the 30-week RM recruit training course. Institute of Naval Medicine, 2001 2001.009.
4. Fallowfield J, Wilkinson D. A review of the progressive nature of physical conditioning to train Royal Marine Commandos. Gosport: The Institute of Naval Medicine, 1998.
5. Pethybridge R, Shariff A, Pullinger N, Allsopp A. Statistical evaluation of Royal Marine recruit selection criteria. Institute of Naval Medicine, 2000 2000.033.
6. Hagberg JM, Moore GE, Ferrell RE. Specific genetic markers of endurance performance and VO2max. Exerc Sport Sci Rev. 2001;29(1):15-9. PubMed PMID: 11210441. Epub 2001/02/24. eng.
7. Bilzon J, Gill C, Dalzell J, Allsopp A, Williams C. Influence of military clothing ensemble on the metabolic response to prolonged running in a warm environment. Journal of Sports Sciences. 2001;19:626-7.
8. Allsopp A. Improving the selection of candidates for Royal Marine Recruit training by the use of a combination of performance tests. Royal Naval Medical Service. 2004;90(3):117-24.
9. Wilkinson D, Allsopp A, Childs R, Shariff A. A review of the revised common recruit course syllabus to train Royal Marine Commandos. Institute of Naval Medicine, 1999 99038.
10. Wilkinson DM, Rayson MP, Bilzon JL. A physical demands analysis of the 24-week British Army Parachute Regiment recruit training syllabus. Ergonomics. 2008 May;51(5):649-62. PubMed PMID: 18432443.
11. NATO. Final report and resource manual on military physical training. 1994 NATO Techical report AC/243 (Panel 8) TR/16.
12. Munnoch K, Bridger RS. Smoking and injury in Royal Marines' training. Occupational medicine. 2007 May;57(3):214-6. PubMed PMID: 17218331.
13. MoD. Human Factors for Designers of Equipment, Part 3: Body Strength and Stamina. MOD Defence Standards DEF STAN 00-25 (Part 3/Issue 2); 1997.
14. Jones BH, Thacker SB, Gilchrist J, Kimsey CD, Jr., Sosin DM. Prevention of lower extremity stress fractures in athletes and soldiers: a systematic review. Epidemiol Rev. 2002;24(2):228-47. PubMed PMID: 12762095. Epub 2003/05/24. eng.
15. Friedl KE, Evans RK, Moran DS. Stress fracture and military medical readiness: bridging basic and applied research. Med Sci Sports Exerc. 2008 Nov;40(11 Suppl):S609-22. PubMed PMID: 18849874. Epub 2008/10/14. eng.
16. Armstrong DW, 3rd, Rue JP, Wilckens JH, Frassica FJ. Stress fracture injury in young military men and women. Bone. 2004 Sep;35(3):806-16. PubMed PMID: 15336620. Epub 2004/09/01. eng.
17. Dixon S, Cready M, Allsopp A. Comparison of static and dynamic biomechanical measures in military recruits with and without a history of third metatarsal stress fracture. Clinical Biomechanics. 2006;21:412–9.
18. Moran DS, Heled Y, Arbel Y, Israeli E, Finestone AS, Evans RK, et al. Dietary intake and stress fractures among elite male combat recruits. J Int Soc Sports Nutr. 2012;9(1):6. PubMed PMID: 22413851. Pubmed Central PMCID: 3382422. Epub 2012/03/15. eng.
19. Birrell SA, Hooper RH, Haslam RA. The effect of military load carriage on ground reaction forces. Gait Posture. 2007 Oct;26(4):611-4. PubMed PMID: 17337189. Epub 2007/03/06. eng.